![]() Yes, you read that correctly. Says Ron Shemenski, a former physician for the station, “We were stuck in a place that’s harder to get to than the International Space Station. We know we’re on our own.” A sick astronaut on the International Space Station can jump in the return vehicle permanently parked at the station and make it back to earth in about 3.5 hours. In contrast, just to get a plane to the Amundsen-Scott South Pole research station takes 5 days – in good weather. Which is not at all the situation right now – at the South Pole it’s the very middle of winter.
Yes, you read that correctly. Says Ron Shemenski, a former physician for the station, “We were stuck in a place that’s harder to get to than the International Space Station. We know we’re on our own.” A sick astronaut on the International Space Station can jump in the return vehicle permanently parked at the station and make it back to earth in about 3.5 hours. In contrast, just to get a plane to the Amundsen-Scott South Pole research station takes 5 days – in good weather. Which is not at all the situation right now – at the South Pole it’s the very middle of winter.
 This makes for an incredibly risky evacuation. It’s so risky that the scientists at the station expect to stay there from February to October, no matter what. The on-site physician biopsied and administered chemotherapy to herself in 1999. A scientist who suffered a stroke in 2011 had to wait until the next scheduled flight. However, winter medical evacuations have been performed twice before in the history of the station (since 1957), in April 2001 and September 2003. These two evacuations were performed by the same company that will perform this rescue. On June 14, the National Science Foundation (who runs the station) approved the medical evacuation of a scientist there. Two flights left Calgary, Canada that same day.
This makes for an incredibly risky evacuation. It’s so risky that the scientists at the station expect to stay there from February to October, no matter what. The on-site physician biopsied and administered chemotherapy to herself in 1999. A scientist who suffered a stroke in 2011 had to wait until the next scheduled flight. However, winter medical evacuations have been performed twice before in the history of the station (since 1957), in April 2001 and September 2003. These two evacuations were performed by the same company that will perform this rescue. On June 14, the National Science Foundation (who runs the station) approved the medical evacuation of a scientist there. Two flights left Calgary, Canada that same day.
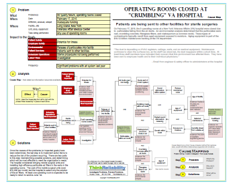
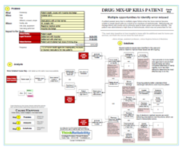
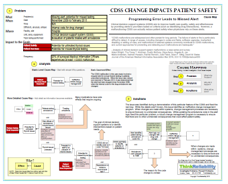
What makes the evacuation so risky that there is a debate over whether or not to rescue an ailing scientist? There are multiple factors that are considered in the decision. These issues can be developed within a cause-and-effect diagram, presented as a Cause Map. The first step in the process is to determine the impacts to the goals that result from a problem. In this case, we will look at the problem of a scientist at the South Pole becoming ill and requiring evacuation. There is an impact to the patient safety goal due to the delay of medical treatment. There’s also an impact to the safety of the aircrew on the flights used to rescue the scientist. There’s also an impact to property/ equipment and labor/ time due to the risky, complex evacuation process.
In the analysis (the second step of the process), the impacted goals become the effect in the first cause-and-effect relationships. The delay in medical treatment for the patient (the ailing scientist) results because required treatment is not available at the station, although a physician and physician’s assistant staff the clinic throughout the winter. There’s also a delay for the decision to send an evacuation plane. In this case, a day and a half of deliberation were required. As previously discussed, normally planes do not arrive at the station during the winter. It’s happened only twice previously in the last nearly 60 years. In order to ensure safety, the crew at the station undergoes a rigorous medical screening, to prevent illnesses requiring evacuation as much as possible.
Medical treatment is also delayed by the time required for the plane to arrive at the South Pole, and then for the plane to return the patient to a medical treatment center. (Which center is determined by the nature of the medical issue, which has not been disclosed, but the nearest centers are thousands of miles away.) The trip to the South Pole takes at least 5 days because of the complexity of the process. It also poses a risk to the air crews making the trip. (There are two planes sent in; one for evacuation and one to remain nearby in a search-and-rescue capability.)
The conditions in Antarctica are the cause of many of the difficulties. The sun set at the station in March, and will not rise again until September, so the plane must land without any daylight. It also has to land on packed snow/ ice, which requires skis, as there are no paved runways and the average winter temperature is -76°F (with wind chill it feels like -114°F). At those temperatures, most jet fuel freezes, so only certain planes can make the trip. (This is why they’re coming from Canada.) The planes can only hold 12-13 hours of fuel, and the last leg of the trip (across Antarctica) takes 10 hours (again, in good weather) so after a few hours into the flight, the plane has to either turn back, or they must land at the South Pole, regardless of conditions. Due to the desolation of the area, there’s nowhere else to land or refuel.
Currently one plane has made it to the South Pole, where it will wait for at least ten hours to allow the flight crew to rest and monitor the weather. The second plane remains at the Rothera Research Station, on Adelaide Island on the edge of Antarctica. Check for updates by clicking here. View the one-page downloadable Cause Map by clicking “Download PDF” above.